1. Introduction
Responding effectively to an unprecedented health crisis like the COVID-19 pandemic with several “unknown unknowns” is a daunting task for several governments. Uncertainty plagues strategic governance decisions amid coronavirus crisis. Yet, publics expect the authorities to live up to expectations especially when the crisis is transboundary and involves rapidly metamorphosing events (Ola & Zeger, 2020). In such complicated and ambiguous situations, developing countries plagued with problems of governance may be entangled in policy paralysis and do not fully appreciate the unfolding risk which could lead to disastrous consequences (Idowu, 2020).
The coronavirus pandemic threatens to disproportionately affect the least developed countries with potentially dire consequences for human health and the economy (UN, 2020; World Bank, 2020b). The West Africa Ebola epidemic that quickly over-whelmed the health systems of Sierra Leone, Guinea and Liberia is a fresh reminder of the vulnerability of developing countries to epidemics (Moon, et al., 2015). Many African countries have fragile health systems not well-equipped to deal with COVID-19 (Bang et al., 2020). For instance, 10 African countries have no ventilators while just 2,000 ventilators are available for the 41 least-resourced African countries (Maclean & Marks, 2020). Hence the ramifications of the pandemic could be profound and long-lasting in the continent where the health systems of most African countries are permanently in crisis (Waal, 2020), worsened by weak governance (Idowu, 2020).
Governance policies in response to epidemic diseases in many African countries could affect governance more than the epidemics themselves. For instance, infection control measures during epidemics could be unpopular creating mistrust that could lead to resistance in the population. This was the case in 2014 during the Ebola virus when the Liberian government’s attempt to lockdown the capital Monrovia resulted to fierce resistance (Moon, et al., 2015). Just like in Sierra Leone and Guinea, conspicuous governance challenges existed in national coordination of the Ebola epidemic response including fast detection, infection tracing, basic care, and quarantine of patients (Madhav, 2018). Furthermore, enforcing lockdown or infection control measures through health-related emergency powers often lead to accusations of abuse of power (Waal, 2020).
Managing the coronavirus pandemic in Africa would require innovative governance approaches. The WHO provided the International Health Regulations (IHR) that sets a framework for countries to detect, monitor, report and respond to infectious disease outbreaks (WHO, 2008). Despite these efforts, progress towards achieving the IHR has been slow in developing countries where serious inadequacy in pandemic preparedness, governance, leadership, and funding abound (Looke, et al, 2015; Damme, et al., 2018). Consequently, the WHO underscored the relevance of research into the role of governance in public health emergencies in low- and middle-income countries (WHO, 2018a). This research endeavour make a modest contribution to this end by exploring Cameroon’s governance of the COVID-19 pandemic since the country is one of the most affected in Africa (OCHA, 2020).
This research seeks to examine the COVID-19 pandemic crisis management in Cameroon with the overarching aim of assessing the role of governance in the overall crisis response. The central goal is to understand whether Cameroon’s governance strategy would be able to engineer an effective health response as the health crisis prolongs. The outcome of the research has informed recommendations for improvements in the subsequent response to the crisis.
2. Brief Overview of Cameroon’s Health Profile
Cameroon’s risk profile is overburdened with health hazards including natural, potentially socio-natural, technological, social, and anthropogenic hazards (Figure 1B; Bang et al., 2019). Cameroon is a Lower Middle-Income bilingual country (English and French as official languages) found along the Atlantic Ocean between Central and West Africa with a population of around 26 million people (2019 estimate) spread over 10 administrative regions ( Figure 1A). The country has a poverty rate of 44.7% and life expectancy of 58.9 years at birth (World Bank, 2020a).
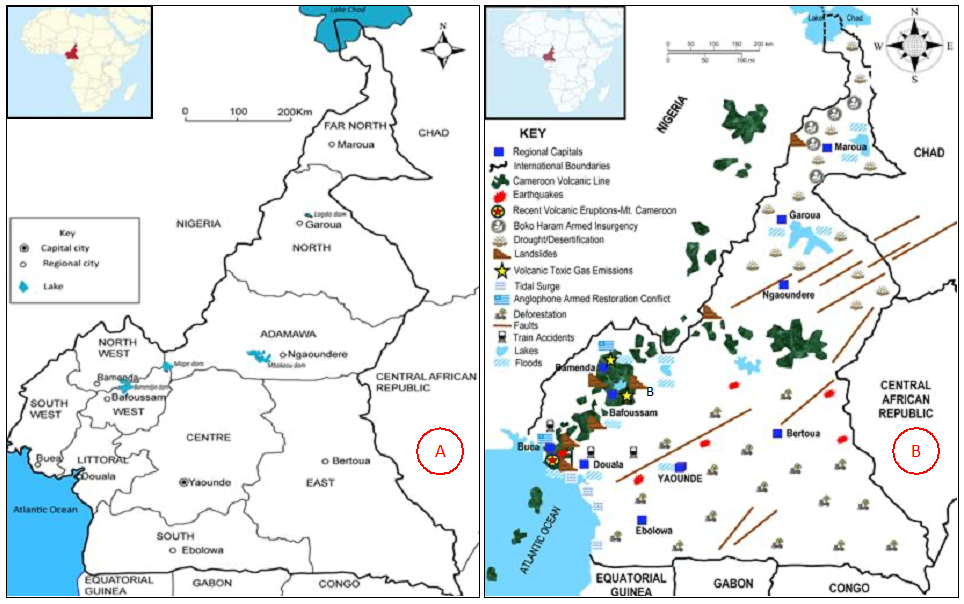
Figure 1. Maps of Cameroon (A) showing the 10 administrative regions and their capital cities and (B) Location of the main hazards in the country.
Sources:(A) Ndi and Kimengsi (2017) and (B) Bang et al. (2019).
2.1 Cameroon’s health structure
Prior to independence in 1960, Cameroon’s health system was designed to serve the colonial administrators in urban areas to the detriment of rural areas where most of the populace lived (Molem, 2008). After signing the Alma Ata Declaration (AAD) in 1982 that introduced primary health care reforms, the government has pursued a decentralised health policy albeit with limited implementation (WHO, 2016). Theoretically, Cameroon’s health system is structured to work at three levels (Central, Intermediate and Peripheral) following a top down hierarchical order (Table 1). The co-financing of primary health care between the government and the community, as enshrined in the AAD is skewed with the latter bearing most of the cost ( around 70.4% of the health expenditure; WHO, 2016). Hence, most Cameroonians cannot afford the excessive cost of health care, including health insurance (Nde et al., 2019), restricting access to health services including treatment for COVID-19 (HRW, 2020).
Table 1. The top-down structure of Cameroon’s Health System.
|
Level |
Administrative Structures/Units |
Competencies/Functions |
Healthcare Facilities |
Dialogue Structures |
|
| |
Central |
MPH & associated Central Services (Secretary General, Secretary of State, Technical Departments) |
Policy Formulation, Development of Strategies, Regulation, Coordination, Supervision |
Referral Hospitals, General Hospitals, Central Hospitals, University Teaching Hospital, NCPEDMS, HCRHRES, NLQCD|V, CBRS, CPC, NPHO. |
National Council of Health, Hygiene & Social Affairs; Board of Directors of Management Committees. |
|
Intermediate |
Regional Delegations in the Capitals of the 10 Regions |
Provision of Technical Support to Health Districts & Programmes; Regional Coordination; Regulation & Supervision at the Regional Level |
Regional Hospitals in the capitals of the 10 Regions |
Regional Hospitals, Regional Fund for Health Promotion |
|
|
Peripheral |
189 Health Districts |
Provision of Healthcare Services; District Coordination & Regulation |
Sub-Divisional Medical Centers, District Hospitals, District Medical Centers, Clinic, Integrated Health Centers, Health cabinets, Ambulatory Health Centers |
District Health Centre; District Medical Centre, Sub-Divisional/District Health and Management Committees |
|
|
ACRONYMS: NCPEDMS=National Centre for the Procurement of Essential Drugs and Medical Supplies, HCRHRES=Hospital Centre for Research ,Human Reproduction and Endoscopy Surgery, NLQCDV=National Laboratory for the Quality Control of Drugs and Valuation, CBRS=Chantal Biya International Research Centre, CPC=Centre Pasteur of Cameroon, NPHO=National Public Health Observatory |
|||||
2.2 Burden of disease
The burden of communicable diseases is largely driven by HIV/AIDs, malaria and tuberculosis, while others like diarrheal diseases, respiratory tract infections, hepatitis A/E, typhoid/dengue/yellow fever, African trypanosomiasis, plague, cutaneous leishmaniasis, schistosomiasis, sexually transmissible infections, meningococcal meningitis, rabies, buruli ulcer, Onchocerciasis, geo-helminthiases, rubella, diphtheria, measles, mumps, neonatal tetanus, pertussis also occur across the county. The chronic non communicable diseases are diabetes, cancers (cervical, breast, prostrate), cardiovascular diseases (hypertension) and respiratory diseases (wheeze, asthma) including road traffic/unintentional accidents prominent in urban centers (Echouffo-Tcheugui & Kengue, 2011; WHO, 2016; Papia et al., 2020). Generally, the country has experienced a general decrease in disease burden from 1990-2017 although the rate of decrease for non-communicable diseases has been slower than others (Roser & Ritchie, 2020).
2.3 Cameroon’s health system performance
An evaluation of Cameroon’s Health Sector Performance (HSP) for fifteen years (2001-2015) was done in 2015 based on key health indicators and targeted Health System Strategies (HSS). It paints a bleak picture of Cameroon’s HSP and provides an insight into Cameroon’s health system and its capability to sustain the COVID-19 pandemic.
The public health infrastructure and equipment are not enough and disproportionately distributed across the country leaving District Hospitals with the least resources. The ratio of health personnel (doctors, nurses, midwife, technicians, pharmacist etc.) to the population remains exceptionally low (WHO, 2016). There is stagnation in public funding, life expectancy and regression in areas of maternal mortality, disease control and family planning. The life expectancy at birth in Cameroon was 57.3 in 2015, which is lower than the average for sub-Saharan Africa (60 years) and the world (71.4 years) (NOPH/MPH, 2017).
Non-communicable diseases (NCDs) have been increasing in the country and accounted for a sizable proportion of all fatalities in 2014 (Agbor & Tambi, 2014). Communicable diseases were responsible for a considerable amount of disease burden and deaths in 2013. Not all is gloom though! Considerable progress has been made to reverse the spread of HIV/AID and many more people have access to safe drinking water and basic sanitation. Yellow fever immunization coverage increased from 64.8% to 85.8% (WHO, 2016; MPH, 2016, 2017).
Overall, Cameroon has not achieved the objectives of the HSP due to improper management of financial resources and information, deficient performance of the health sectors, lack of an integrated monitoring/evaluation plan, and deficient accountability methods/processes (WHO, 2016). These deficiencies have implications for the governance and effective response to the COVID-19 pandemic.
3. Theoretical Framework: Comprehensive Pandemic Risk Management System (CPRMS)
A novel conceptual framework, the Comprehensive Pandemic Risk Management System (CPRMS) model (Studzinski, 2020) has provided orientation, structure and focus to the article (Potschin-Young, et al., 2018). The CPRMS is underpinned by governance elements suitable to gauge epidemic/pandemic response; is grounded in empirical evidence; adopts a multisectoral/multidisciplinary approach; takes an integrated approach to pandemic risk management; embraces a risk management approach; integrate prevention, preparedness, and response measures and has secular scope (Studzinski, 2020).
Indeed, the CPRMS supports a well-coordinated and organized effort to implement operational policies, plans and strategies from the local to global level. The framework has three core components (see Figure 3): (1) pandemic risk spectrum in hierarchical order; (2) critical infrastructure and essential services and (3) a multisectoral institutional framework underpinned by six strategic system building blocks (SBB). The six SBBs are (1) Governance/Leadership and Coordination; (2) Human Resources; (3) Financing; (4) Information systems (coordinated generation and distribution of data, information, knowledge); (5) Operational Interventions/Service Delivery and (6) Essential Commodities/Logistics.
The model encapsulates a broad view of interrelated and interconnected global, national, and regional dimensions with each geographic realm having its own internal coherence strengthened by the six component building blocks. The relevance and application of the CPRMS to this article anchors on the national geographic realm that applies to a country (Cameroon in this research) in consideration of the six component building blocks along the “Institutional System” axis (Figure 2). The CPRMS, therefore, provides theoretical/conceptual and practical understanding and guidance on pandemic crisis management with underlying governance strategic management. Hence, its application to the COVID-19 pandemic crisis management in Cameroon in this article.
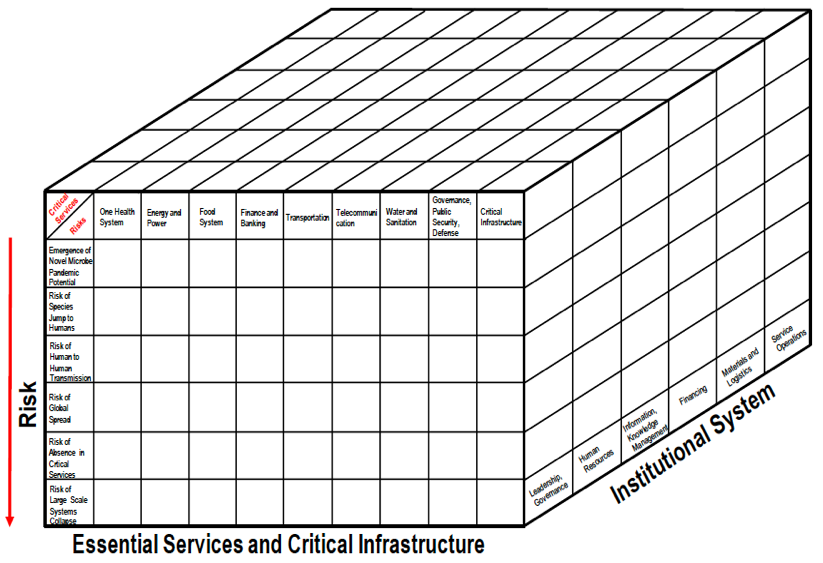
Figure 2. Three-dimensional representation of the Comprehensive Pandemic Risk Management System.
Source: Adapted from Studzinski, (2020)
4. Methodology
This research is principally qualitative, exploratory, and descriptive (Reiter, 2017) to unveil initial insights into Cameroon’s management of the COVID-19 pandemic. Initial attempts to collect empirical data from senior/top government officials dealing with the pandemic response was difficult. Other than their hectic schedules which does not provide much room to grant interviews, the authorities are reluctant to comment on governance strategies they perceive to be dynamic in response to the evolving pandemic crisis. Hence primary/secondary data were used to inform this research.
In circumstances where collecting empirical data is difficult, primary information becomes an invaluable source of data especially in unfolding incidents (Kabir, 2016) like the COVID-19 pandemic. Government primary sources of data on COVID-19 management was obtained from government/official policies, plans and programmes; inter-agency/ministerial press briefings, reports, circulars, guidelines, communiques, and statements published on the websites of stakeholder government agencies/ministries—MPH, Ministry of Territorial Administration (MTA); Ministry of Communication (MCOM), Ministry of Transport (MT), Ministry of Telecommunication (MTEL) etcetera.
The COVID-19 policies, plans, programs, project, and country/situation report of international and humanitarian agencies liaising with the Cameroon government to combat COVID-19 complemented the primary data sources. Notable are the World Health Organisation (WHO), United Nations Development Programme (UNDP), UN’s Office for the Coordination of Humanitarian Affairs (OCHA), International Organisation of Migration (IOM); World Food Programme (WFP), Cameroon Centre for Disease Control and Prevention (CDC), Norwegian Refugee Council (NRC), International Medical Corps (IMC), Central Emergency Response Fund (CERF), French Red Cross (FRC), Lutheran World Federation (LWF) Médecins Sans Frontieres (MSF) etcetera. These ministries, agencies and organisations have regularly uploaded COVID-19 documents and reports on their websites that informed the research (Hammarberg et al., 2016; Rapley, 2016; Bhattacherjee, 2012).
Secondary data was obtained from scholarly articles and grey-literature sources. The paucity of the former is noticeable since the pandemic is just a few months old, thereby, underlining the relevance of grey sources (local, national and international media ) to inform knowledge on the unfolding crisis (White, et al., 2013; Hammarberg et al., 2016). Content analysis was used to peruse and categorise the data sources into relevant themes (Bryman, 2004) guided by the SBBs of the CPRMS framework.
5. Findings
The six component SBBs of the Institutional System in the CPRMS (see Figure 2) informed the thematic analysis and have elicited knowledge on the pandemic response presented in the findings.
5.1 Governance of the COVID-19 response
The governance aspects discussed in this section are leadership, institutional arrangements and administrative decisions, briefings and decentralisation.
5.1.1 Leadership
Cameroon’s response to the COVID-19 pandemic is under the leadership of the President of the Republic, delegated to the Prime Minister (PM), Head of Government. Efforts to convince the population that the government is fully in charge of the pandemic managements was undermined from the top of the governance structure. Cameroon’s 87-year-old President was not seen or heard from for 35 days after the Prime Minister (PM) announced government’s initial measures to tackle the pandemic on March 17, 2020. This was a critical period at the beginning of the pandemic when citizens all over the world were getting assurance from their presidents and daily briefings on measures to combat the virus. Due to pressure from the main opposition party, the president addressed the nation for the first time on April 16 amidst heavy criticisms from Cameroonians for being quiet and widespread speculations on social media about reasons for his prolonged absence despite the country being one of the hardest hit by COVID-19 in Africa (Krishnan, 2020).
5.1.2 Institutional arrangements
The Cameroon government’s response strategy for the COVID-19 pandemic is in accordance with the administrative governance of the country by different echelons of government at the national, regional, and local (Divisional/District) levels. The PM heads an Inter-Ministerial Committee in charge of monitoring and evaluating the implementation of government’s response strategy to the coronavirus pandemic (Republic of Cameroon, 2020c). The Ministry of Public Health (MPH) is the lead agency responsible for coordination the coronavirus response strategy and policy at the national level. Stakeholder ministries liaising with the MPH include MTA, MCOM, MT, MTEL etcetera. In accordance with Cameroon’s top-down administrative governance structure, the ten Regional Delegates of Public Health and stakeholder ministries are responsible for COVID-19 management in their areas of authority. Operationally, the regions/districts are not enhanced and sufficiently empowered to manage the COVID-19 response (UNICEF, 2020).
5.1.3 Administrative decisions
The first cases of COVID-19 in Cameroon was reported on March 6, 2020 and since then, the Cameroon government has progressively implemented a series of containment measures. The first official government response via the PM on March 17, 2020 saw the announcement of a set of 13 measures to mitigate the virus spread. In less than two months after the initial measures, the number of infections had skyrocketed to 2,077, with 245 deaths (Worldometer, 2020) indicating an exponential increase in the number of cases. The real number of cases/deaths are far higher because diagnosis is inadequate with limited coverage all over the country (Bang et al., 2020; OCHA, 2020). Subsequent restrictive measures, decrees, policies, plans had been announced to complement the initial measures (see Table 2) albeit most were eased just after 6 weeks amidst concerns the infection rate was escalating (Tamfu & Lietbouo, 2020).
Table 2. The main COVID-19 strategies, policies, plans, or actions taken by the government from March-July 2020.|
Themes |
Government Decisions, Actions, Policies, Strategies |
|
Governance & Accountability |
Coordinate COVID-19 activities in the public and private sectors. |
|
Ensure resources for managing the pandemic are used efficiently. |
|
|
Ensure transparency in managing resources for the pandemic response. |
|
|
Creation of $1 billion COVID-19 response solidarity fund on April 1, 2020. |
|
|
President’s appeal for Cameroonians to respect government’s response measures. |
|
|
Decentralisation of the COVID-19 response to the regions on April 20th, 2020. |
|
|
Order prohibiting the raising of funds for the pandemic without authorisation from the MTA. |
|
|
Ministerial order to close accounts opened to raise funds for the pandemic without from the MTA. |
|
|
Order by SDO of Leke Division prohibiting the distribution of COVID-19 materials without authorisation. |
|
|
External Infection Control & Basic Services |
Cameroon’s land, air and sea borders were temporarily closed. |
|
Implementation of COVID-19 safety/preventive measures at points of entry into Cameroon. |
|
|
Temporary stop of visa issuing at all entry points into the Cameroon. |
|
|
Travelers entering Cameroon mandated to complete a health declaration form. |
|
|
Temporary suspension of Cameroon’s para-public sector/diplomatic missions abroad. |
|
|
Restrictive border measures allowed essential goods/essential into the country. |
|
|
No restrictions on internal transport to allow circulation of essential services and goods. |
|
|
Repatriation of Cameroonians stranded abroad. |
|
|
Internal Infection Control Measures |
Face masks made mandatory in all public spaces and means of transport. |
|
Temporary closure of all educational/training institutions and sporting activities throughout the country. |
|
|
Sanctioning of populace that fail to respect restrictive/confinement measures. |
|
|
Temporary prohibition of gatherings of more than fifty people throughout the country. |
|
|
Opening times for restaurants, bars and entertainment facilities restricted to 6 pm. |
|
|
Business premises to implement infection control measures. |
|
|
Public administrations urged to have virtual/digital meetings. |
|
|
Pledge for search of COVID-19 patients through massive testing. |
|
|
Raising awareness about the pandemic via many platforms and sources |
|
|
Setup of emergency COVID-19 toll-free hotline number (1510) |
|
|
Presidential decree of April 15, 2020 commuting and remitting prison sentences. |
|
|
Set up of few quarantine and treatment centers in some regional capitals. |
|
|
Requisition of private health facilities essential to implement COVID-19 response. |
|
|
Order from the Governor of the Littoral Region prohibiting on-the-spot consumption of drinks. |
|
|
Order from SDO of Menoua Division prohibiting corpses from entering his Division and the burial of people who die within the Division at their place of death. |
|
|
Scaling Up Measures |
Specialized treatment centers to be established in the regional capitals. |
|
Establishing and increasing testing in all the 10 regions of the country. |
|
|
Sensitisation to be done in Cameroon’s official and vernacular/indigenous languages. |
|
|
Pledge to intensity COVID-19 screening, and awareness raising campaigns, acquire essential hospital equipment and encourage local production of essential COVIC-19 materials. |
5.1.4 Crisis Management Briefing
The Minister of Public Health have held several meetings with other government, local and international stakeholders in the public and private sectors, including international and humanitarian agencies and the diplomatic services to address the COVID-19 response (OCHA, 2020; CRTV, 2020a). At the onset of the response, there were daily briefings mostly in French on the rapidly evolving coronavirus epidemiological situation concerning infection rates, cured cases, fatalities, and government strategy. The regular briefings, however, were stopped abruptly less than three months after the containment measures and the Minister reverted to providing information online via the MPH’s website. Whilst the reason to stop open press briefing was not mentioned, sceptics believe it may be related to concealing the higher death toll from the virus (APA, 2020).
5.1.5 Decentralisation
Government’s decentralisation strategy is aimed to optimize the autonomous management of the pandemic in all the 10 regions of the country for rapid and efficient care of patients since the limited critical care and testing facilities were overly centralised in Yaoundé and Douala. In consultation with civil society actors, parliamentarians and other international stakeholders assisting in the pandemic response, the government announced a series of measures to decentralise the pandemic management to the regional/local levels on April 9, 2020. Notable, was the establishment of treatment centers for COVID-19 patients in all the 10 regional capitals (Republic of Cameroon, 2020a). The decentralisation strategy, theoretically, could enhance regional/local response to the pandemic. Its success, however, will depend on government’s political commitment to provide the required health resources/facilities.
5.2 Resources for COVID-19 response
The resources addressed here are health/human resources and financial/material resources.
5.2.1 Health facilities/ human resources
Cameroon’s health infrastructure/facilities are inadequate (Cabrol, 2018) and unsuitable to effectively respond to the COVID-19 pandemic (Bang et al., 2020). The health infrastructure is acutely inadequate and disproportionately distributed in the country (HRW, 2020; OCHA, 2020). An assessment of Cameroon’s public health infrastructure shows that 30.1 % of the medical facilities are either in Yaoundé or Douala (WHO, 2016). Indeed, the health facilities in Yaoundé and Douala are servicing 34.5% of Cameroon’s population (based on the 2015 population of around 20,504,419). More than half of the pharmacies in the country and specialised services such as Ophthalmology, Hemodialysis and Imaging units are either absent or poorly distributed around the country (WHO, 2016). The inadequate, limited, and disproportionate distribution of the health facilities limits health care accessibility to Cameroonians at the regional and local levels.
5.2.2 Financing/material resources
Research evidence suggests the Cameroon government needs substantial financial and technical assistance to fight the coronavirus pandemic (Bang et al., 2020). Consequently, the government created a National Solidarity Fund to finance the pandemic operations (MTA, 2020) and the MPH, launched a website to receive public donations (MPH, 2020a). Assistance has been pouring in from many sectors (Table 3). In early May 2020, the IMF, under its Rapid Credit Facility (RCF), disbursed US$ 226 million to the Cameroon Government to aid in the coronavirus combat (IMF, 2020). Despite the assistance, medical facilities continue to experience shortages in basic hospital goods for COVID-19 treatment like glasses, gloves, masks, disinfectants, protective gear for nurses/doctors, thermometers, medicines including ventilators and oxygen (HRW, 2020; Bang et al., 2020).
Table 3. Some sources of donations/help for the pandemic response in Cameroon.|
Source of Assistance |
Support/Assistance Provided |
|
WHO |
Medical consignment and capacity development for health workers. |
|
OCHA |
Capacity development (training/recruitment) for health workers. |
|
CERF and UNDP |
Protective gear (medical masks) for health workers. |
|
Chinese Billionaire |
Large consignment of medical equipment. |
|
UNDP |
Medical equipment worth FCFA 2.3 billion. |
|
WFP |
Several humanitarian flights |
|
U.S. CDC |
Technical Support |
|
Plan International, IMC, NRC, FRC, LWF, |
Handwashing kids to communities; Community engagement, Risk communication and awareness; Water sanitation and hygiene; Training of community health workers. |
|
UNICEF |
Technical and financial support for awareness-raising; Facilitated the revision of the MPH’s COVID-19 communication documents |
|
UNHCR |
Sensitisation on preventive measures and provision of rapid tests, handwashing, temperature checks in refugee camps. |
|
MSF |
Enhancing health capacity all over the country (triage, infection prevention and control measures, increasing hospital capacity). |
|
USAID |
Supported the MINSANTE to model the COVID-19 epidemic to better understand and quantify needs. |
|
British Government |
Financial support to decentralise testing |
|
IMF |
Provided credit worth US$ 226 million) |
|
CSI |
Distribution of masks and hydroalcoholic gels |
|
CDC Cameroon |
Helped MPH develop COVID-19 preparedness and response plans; Training at national and regional levels; Donated laboratory supplies to the Public Health Laboratory |
|
NRC=Norwegian Refugee Council; IMC=International Medical Corps; CERF=Central Emergency Response Fund; WFP=World Food Programme; WHO=World Health Organisation; UNDP=United Nations Development Programme; OCHA= UN’s Office for the Coordination of Humanitarian Affairs; FRC=French Red Cross, LWF=Lutheran World Federation; MSF=Médecins Sans Frontieres; CDC=Centre for Disease Control and Prevention; CSI=Cameroon Survival Initiative |
|
Many humanitarian/international organisations/NGOs have provided technical assistance, to the government. For instance, the WHO and many NGOs in collaboration with the MPH have been organising COVID-19 capacity building programmes (workshops and training) for health workers in all regions of the country (OCHA, 2020; UNICEF, 2020). Cameroon’s National Public Health Laboratory constructed by the CDC is facilitating COVID-19 specimen collection, transport, and distribution of coronavirus test kits; reporting of results from the decentralised laboratories and assisted to develop Cameroon’s laboratory plans to decentralise the diagnostic capacity of COVID-19 covering all the ten regions (CDC, 2020). Without these assistance, Cameroon may not cope with the response.
5.2.3 Politicising donations
Notwithstanding the dire need for assistance to fight COVID-19, there are concerns that the government has attempted to choke some donations. For example, the Minister of Territorial Administration closed the COVID-19 fundraising accounts of Cameroon’s main opposition party—Cameroon Renaissance Movement (MRC) (LeMonde & AFP, 2020). In another incident, the Minister of Public Health rejected a donation of 950 Covid-19 screening tests and 16,000 protective and surgical masks from the MRC. Furthermore, the MRC’s volunteers were arrested for distributing free face masks and hand sanitizers in Yaoundé (Allegrozzi, 2020). The government claims these measures were taken due to non-compliance with the country’s legally prescribed donation process. However, the government received a contribution of FCFA 20 million ($ 36,100) from the Mfoundi Section of the ruling CPDM party (MPH, 2020b) sparking nationwide disquiet on the need for an all-inclusive policy that allows all pollical parties to participate in the response to the pandemic.
5.3 Information systems on the COVID-19 pandemic response
The relevant aspects discussed under this theme are the Public Health Emergency Operations Centre, situational awareness and community information dissemination and health education.
5.3.1 Public health emergency operations center (HEOC)
Cameroon’s operational ability to manage health crises was boosted in 2018 with the inception of a new Public Health Emergency and Operations Center (HEOC) in the nation’s capital, Yaoundé—funded by the US government (Figure 3A). The HEOC with modern state-of-the art equipment can serve as Incident Command Centre (ICC) to proffer standard operational procedures (SOPs) in managing public health risks, determine and harmonise strategic areas for health intervention, support the development and response plans for health hazards, and facilitate the integration of health resources (US Embassy, 2018; Emmanuel, 2018). The HEOC has been coordinating the COVID-19 pandemic crisis response, serving as the national ICC for the entire nation (CRTV, 2020b). Some regions have also created COVID-19 ICCs (Figure 3B). The relevance of regional ICC became more apparent when the government decentralised the pandemic response to the regional level.

Figure 3. (A) Inauguration ceremony of Cameroon’s Public HEOC located in Messa, Yaoundé on December 3rd, 2018. Source: Emmanuel (2018);
(B) Sign of the Covid-19 Incident Command Centre in Bamenda, North-West region. Source: (HRW, 2020)
5.3.2 Situational awareness
Situational awareness involves active information gathering, analysis, integration, interpretation validation and sharing that helps to strengthen public health operational ability/capacity to support decision making across critical infrastructure sectors and all levels of government before, during and after an incident (Madhav, 2018; ASPR, 2015). The HEOC has facilitated situational awareness for the pandemic response through facilitating the collection, harmonisation and analysing COVID-19 bio surveillance data across the country and updating knowledge on the infection and spread rate of coronavirus. This has been facilitating government resource mobilisation, distribution and utilisation. The HEOC has played a fundamental role to capture, disseminate and coordinate health information at the national and regional levels that has informed governance decision on the evolving COVID-19 health risks.
5.3.3 Community information dissemination and health education (CIDHE)
Community information dissemination and health education (CIDHE) for COVID-19 has been done in Cameroon via multiple platforms and channels including TV, radio, print media, flyers, posters, the MPH’s website, health facilities, volunteers, community health workers, social media, family and friends (IOM, 2020; OCHA, 2020; IPSOS, 2020).
The messages being disseminated include COVID-19 symptoms, infection, transmission, protection, safety, and hygiene measures. (Figure 4; MPH, 2020a; IOM, 2020; OCHA, 2020).

Figure 4. Some CIDHE flyers on the website of Cameroon’s Ministry of Public Health.
The main actors/agencies involved in CIDHE are the MPH, MICOM and several NGOs. According to the UN Office of Humanitarian Affairs, around 17,138,607 Cameroonians had accessed CIDHE by June 2020 (OCHA, 2020), which is around 66% of Cameroon’s population (2019 estimate). An IPSOS survey also found that around 97% of Cameroonians have heard of the pandemic (IPSOS, 2020).
The high population accessibility to CIDHE, however, is not proportionate across the country. The availability, easy accessibility, dissemination, and coverage of CIDHE varies. According to the IOM just 49% of entry points into Cameroon had COVID-19 information as of April 2020 (IOM, 2020). In addition, the United Nations estimates that only 46% of the population in the conflict-ridden Anglophone Regions have access to information required for the prevention of COVID-19 (OCHA, 2020). The evidence also points to conflicting messages from the social media. For example, analysis from an IPSOS survey revealed that Cameroonians believe Africans cannot be infected with the disease (22%); hot climate prevents the spread of COVID-19 (60%); the virus can be prevented via drinking lemon and vitamin C (66%) and that it can be cured with garlic (50%) or drinking bleach (9%) (IPSOS, 2020b). In recognition of these myths, the CDC has been engaging with the populations in some regions to counteract COVID-19 misinformation (CDC, 2020). Nevertheless, more targeted CIDHE is needed to mitigate the impact of these myths.
5.4 Operational interventions/service delivery for COVID-19 response
The sub-themes examined in this section are scaling up service delivery, trust in the health system and traditional treatment.
5.4.1 Scaling up service delivery
The authorities have limited ability to scale-up COVID-19 intervention coverage all over the country. The difficulty to rapidly expand health system services to accommodate a rise in the number of COVID-19 patients is contingent on the poor health infrastructure and the inability of the system to deploy enough specialist health personnel and equipment to all the 10 regions. Not all the administrative regions have laboratories for testing COVID-19 and the capacity for some had been exceeded (OCHA, 2020). Theoretically, the government scaled-up its intervention to the entire country through the decentralisation policy as mentioned earlier. The appropriate resource to actualise the policy is yet to be provided. Through financial, technical, and material assistance from local and international partners, COVID-19 service delivery in capacity development and the provision of basic health equipment and PPE is gradually being scaled-up in the regions (Bang et al., 2020; UNICEF 2020; Cameroon Tribune, 2020; MSF, 2020). Despite these efforts, treatment for COVID-19 patients at the regional levels remains ineffective due to lack of intensive care units (Bang et al., 2020).
Although the government has made COVID-19 testing free, the population is still being charged for all associated treatment, which is costly. Limited access to health insurance for Cameroonians and the excessive cost of treatment could be a disincentive to seek COVID-19 care (WHO, 2016; HRW, 2020). Even in non-crisis times, 64% of Cameroonians do not seek healthcare due to the excessive cost (Nde, et al., 2019).
5.4.2 Trust in the Health System
The evidence suggests that trust in Cameroon’s CIDHE and in the health facilities to treat COVID-19 is low. A recent empirical study revealed the Cameroon public lacks complete confidence and/or trust in the health system (Bang et al., 2020). This is justified by an earlier survey that showed only 55% of Cameroonians trust government’s CIDHE while 45% feel they need more information on cure, personal/family protection, how the virus spreads and how people can be infected (IPSOS, 2020). Furthermore, there are reports of Cameroonians avoiding hospitals for fear of being infected with the virus and hundreds of patients hospitalised for other diseases have fled from hospitals for fear of being infected with COVID-19. This was confirmed by the Public Health Minister who disclosed that patients fled without completing their treatment (Kindzeka, 2020). The authorities need an aggressive public sensitisation campaign to change public perception and restore confidence in the health system. Depleting trust in the health system has made many Cameroonians to resort to alternative treatments for coronavirus.
5.4.3 Traditional treatment for COVID-19
Traditional medicine seems to be filling the void created by lack of trust in the health system. Cameroonians have been flooding the Douala diocese of the Catholic Church to seek COVID-19 treatment from an Archbishop (Samuel Kleda) who claimed to have developed a plant-based drug for coronavirus and have used it to treat around 3,000 patients (Kouagheu, 2020). The government’s position on the use of non-scientific means to treat coronavirus patients is unclear. The Minister of Health cautioned against the use of traditional medicine while the PM has articulated support for local efforts to develop endogenous remedies for treating coronavirus patients but fell short of encouraging COVID-19 patients to get traditional treatment (Tih, 2020). As patients shift away from the health system, there is a higher risk of more infections and deaths.
5.5 Provision of essential commodities/services and logistics
Whilst instituting border and internal lock-down measures to protect public health, the government ensured essential services and goods were available. The restrictive measures affected at least 65 points of entry (4 airports and 61 land and blue border crossing) into the country (Figure 5). Nevertheless, flights and vessels bringing essential items (food, medication, equipment etc.) into the country were not suspended during the border restrictions. The land border crossings were only partially closed (3 open, 39 partially open and 33 closed ) to allow transportation of goods to Cameroon’s landlocked neighbouring countries (IOM, 2020). This has had implications for cross-border COVID-19 infections.
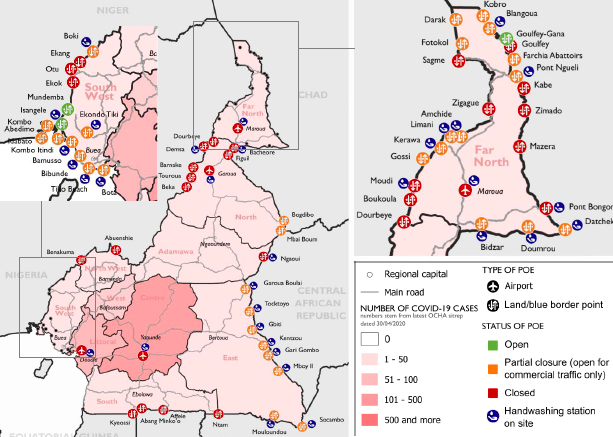
Figure 5. Locations of entry points in Cameroon where COVID-19 restrictions were imposed.
Source: IOM (2020)
Many Cameroonian truck drivers entering the neighbouring countries tested positive for COVID-19. According to the IOM, just around 20% of the entry points into Cameroon were screening travelers for COVID-19 (IOM, 2020). To resolve the problem, Cameroon and Chad held talks and agreed to harmonise COVID-19 testing methods for truck drivers in both countries, and to issue them with test certificate that will be recognised by both countries (OCHA, 2020).
Public transport in Cameroon was not suspended during the lockdown. The rationale was to enable easy circulation of essential services, including health personnel/services and avoid any disruption in the supply chain that would further harm the economy. The transport sector, however, was mandated to follow social distancing measures like overloading of vehicles and wearing face masks.
To ensure the justice system continued to function smoothly during the pandemic, a presidential decree on April 15, 2020 ordered the release of hundreds of prisoners all over the country. Nevertheless, there are allegations that the government continued to arrest and imprison people with minor offences including those exercising their rights to freedom (Offner, 2020). Furthermore, concerns have been raised that sufficient attention has not been given to the needs of the most vulnerable and marginalised people in society like the thousands of IDPs from the Anglophone armed conflict and refugees (OCHA, 2020).
6. Discussion
Timely response was required to prevent the rapidly evolving and unprecedented coronavirus infections from spiraling out of control in Cameroon. The first detected cases in early March were in Douala, Yaoundé and Bafoussam. Had the government sealed off these towns immediately, the virus spread could have been contained. Swift governance actions after outbreak detection of infectious diseases help mitigate the overall effects of the disease (Madhav, 2018; Brattberg & Rhinard, 2011).
From a public heath perspective, the government can be applauded for the strict infection prevention measures. It was difficult to promulgate a strict lockdown considering much thought was not given on managing public expectations and balancing concerns due to the potential socio-economic ramifications to livelihoods (Mbopi-Keou et al., 2020). Cameroon is not a welfare state that can financially support its citizens if they are prevented from generating income since around 90% of Cameroon’s labour force is trapped in the informal sector where the wages are lowest (Kouete, 2020). Attempts to enforce a full and strict lockdown without state support could lead to civil unrest.
The resource limitations experienced during the pandemic and government’s inability to scale-up intervention coverage to accommodate a rise in the number of COVID-19 patients is associated to the poor state of Cameroon’s health infrastructure/system. Pre-emptive preparedness measures would enable easy accessibility to basic medical materials than can be purchased from external sources at the onset of a pandemic.
To ensure sustainable financing during pandemics, Cameroon needs to have risk-based insurance schemes to circumvent the tradition of relying on foreign aid/assistance, which is not guaranteed as donors may also be experiencing significant financial constraints. For instance, the UK foreign aid budget was recently axed by £3bn due to the economic downturn caused by COVID-19 (Crag, 2020).
Over-centralisation of COVID-19 response has implications for containing the virus at the regional/local levels. Rather, strengthening the capacity to identify and diagnose cases at local/community levels would rapidly reduce infection spread. Indeed, decentralised pandemic response is an ideal strategy for effective mitigation of virus spread (Brattberg & Rhinard, 2011; Madhav, 2018). Nevertheless, the community health facilities/units must be empowered to deal with the pandemic.
Politicising and refusing donations from opposition political parties during a crisis when resources are needed is unwise. Crisis governance that inculcates cross-party collaboration should not be seen as the erosion of state power and authority. Opposition parties wishing to assist during a pandemic should not be viewed as potential usurpers of state power. Laying claim to exclusive authority in crisis situations while unable to meet expectations would instead expose authority deficits. An all-inclusive policy/approach to a novel health crisis like COVID-19 would facilitate the response.
Effective communication to the public that is clear, concise with targeted messages is a central pillar of crisis governance. Public communication under unpredictable situations can create anxiety and apprehension for the government as the authorities scramble to contain the pandemic while also communicating with the public on-the-go. Nonetheless, a key focus on CIDHE should be on understanding the messages and targeting the most vulnerable people.
Some infection social control measures are an elusive and unrealistic options for most communities where traditionally, people share common social spaces. Moreover, the inconsistent supply of clean water in most urban and rural areas makes hygienic infection control measures requiring regular had washing unrealistic. Furthermore, poverty is a hindrance to use soap and hand sanitizers as infection control measures.
The governments must contend with the issue of dissipating trust in the health care service. This can be achieved by providing easily understandable narratives and/or expressing reassurance to the population regularly; accurate information dissemination; expressing empathy in messages and anticipatory/measured public communication outings of both desirable and undesirable outcomes (Ola & Zeger, 2020).
So far, Cameroon has been able to sustain the COVID-19 pandemic, thanks to the country’s foreign policy. As the number of cases continue to rise one wonders whether the country would avoid the catastrophic consequences of the pandemic. This article makes a modest contribution to the knowledge on the state of the pandemic five months into the crisis and proffer suggestions (see Table 2) for improvement in governance to avoid potentially calamitous consequences as the pandemic accelerates.
7. Conclusion and Recommendations
The orientation of this research and the structure of this article is underpinned by the six SBBs of the Institutional Systems in the CPRMS model. The coronavirus pandemic constitutes an unprecedented challenge to Cameroon’s healthcare system and the government has demonstrated commitment to combat the virus through the implementation of several crisis responses instruments and strategies albeit much still must be done to get the virus under control.
The findings have revealed significant governance challenges intimately linked to the fragile state of Cameroon’s healthcare infrastructure, which casts a huge shadow over the country’s ability to treat a highly infectious disease like COVID-19. Some governance measures employed to tackle the pandemic leaves much to be desired. Identified constraints exist in the country’s healthcare facilities, resources (financial, human, material) especially in the provision of intensive care for coronavirus patients; centralisation of the response and scaling up interventions in all the regions; politicising contributions from opposition parties, CIDHE that has not sufficiently targeted the vulnerable populace, high cost to access COVID-19 health care; and insufficient trust in the health sector with implications for diverting to traditional treatment for COVID-19.
Currently, one can only speculate on the pandemic’s trajectory but there is no doubt that the threat posed by pandemics has the potential to cause socio-economic turbulence in Cameroon as infections increase and a second wave is predicted. This signals a need for urgent action to bring the virus spread under control.
The identified limitations in responding to the COVID-19 pandemic requires Cameroon to realise that the time is ripe for a paradigm shift in its health system model. The severity of the threat that a pandemic of this caliber possess justifies the need for an overhaul of the public health infrastructure including institutional capacity for pandemic response in anticipation of subsequent health related crisis. Whilst his would be a slow process even under the most optimistic assumptions, political will to initiate change is the first step needed.
Table 4 has recommendations on how to improve the identified challenges in the pandemic response and Cameroon’s health system in the short and long term.
Table 4. Recommendations on how to improve COVID-19 pandemic response and subsequent pandemic crises management in Cameroon.
|
Themes |
Activity |
Recommendation |
|
Governance |
Leadership |
· The president should address the nation immediately at the onset of a crisis to show that topmost leadership is taking control of the situation. · The president should address the nation more frequently in an evolving crisis. |
|
Institutional/Administrative Management & Measures |
· Need to develop multisectoral pandemic risk assessments. · Strategic decision-making meetings/committees should have more social scientists to gauge the societal impacts of measures taken. |
|
|
· After initial cases are detected, containment measures should be swift to prevent disease spread. · Public health safety should be prioritised in decisions to ease lockdown measures to avoid infection rates from rising. · Government should institute a national legislative framework and policy on epidemic/pandemic crisis management that would guide the actions/activities of decision makers/administrators. · Psychological care should be provided for COVID-19 patients and their families. · A data collection and analysis system are needed to check how social measures and public health measures meet local COVID-19 conditions · Contingency plans needed in anticipation of an increasing number of cases. |
||
|
Crisis Management Briefing |
· The government should inform the populace of changes in its briefing program/schedules to avoid speculations. · Providing clear, concise, and regularly updated information is vital to gain public trust and confidence. · Since Cameroon is bilingual (English and French), briefings done in one of the languages should be translated instantaneously into the other language for equal access to the information being communicated. |
|
|
Decentralisation |
· The decentralisation of COVID-19 measures should be provided institutional and legislative support at the regional and local levels. · To operationalise the decentralised management of COVID-19, the required financial, technical, and material resources should be assessed and made available at the regional levels. · The government should build on its coronavirus decentralisation policy to operationalise the complete decentralisation of Cameroon’s health sector to handle later health crises. |
|
|
Resource Provision |
Health Facilities & Human Resources |
· The health infrastructure should be upgraded with more specialist units of larger capacity. · Health facilities with specialist units should be provided in all the regions. · Qualified/specialist health staff should be distributed to key health facilities in all the regions during a pandemic. · More health staff/personnel with adequate training required in the regions. · Employ modelling techniques to foster the quantification of pandemic health-care needs · A more secure and safe working environment for health care workers is required. |
|
Financing & Material Resources |
· Ensure all health districts have regular supply of protective and preventive gear and critical equipment. · Regularly publish updated list of all contributions to ensure accountability. · The diagnostic capacity for infections should be enhanced in the entire country for more accurate monitoring of disease spread. · Contingency plans involving stockpiling of critical materials/medicines would ease patient care at the onset of an epidemic/pandemic. · Need to boost local industry capacity to produce essential equipment like face masks, PPE during a health crisis. · Cameroon needs institutional risk-based insurance schemes to buffer against pandemics. |
|
|
Donations |
· The government should not politicise crises and prevent opposition parties from helping. · Donations from opposition parties should not be rejected when desperately needed. · Government should avoid discrimination in sourcing of funding or logistical support during a crisis. |
|
|
Information Systems |
HEOC |
· Incident Command Centers should be set up in all the regional capitals to facilitate crisis management at the regional levels. |
|
Situational Awareness |
· The government should scale-up bio surveillance and laboratory testing for infection in all regions. · Government should improve its information management ability by harmonising data collection and validation process. · Harmonisation and equal geographic distribution of testing capacity is needed. · Need for more correct and prompt data collection, analysis, and consolidation reporting |
|
|
CIDHE |
· More investment in community sensitisation, health education and mobilization to prevent COVID-19 infections is needed. · More effort should be made to provide CIDHE to the most vulnerable populace during a health crisis. · Need to dispel myths/false information and rumours about COVID-19 |
|
|
Operational Interventions and Service Delivery |
Scaling up service delivery |
· The health system should have the ability to redistribute specialist health personnel and equipment during an epidemic/pandemic. · Scaling up of COVID-19 service delivery to the regions should be associated with an assessment of needs and the provision of appropriate resources. · The cost to access COVID-19 treatment should be free or s subsidised by the government. |
|
Trust |
· Trust building in the populace is needed to encourage more health care access for COVID-19 and the continuation of treatment for other diseases. |
|
|
Traditional Treatment |
· There should be a clear policy on accessing traditional treatment and the government should visa those capable of providing such treatment. |
|
|
Essential Commodities and Services |
· More rigorous screening for infections is needed on the land borders, especially for transporters. · There should be a clear policy to release prisoners during a pandemic, which should prioritise the most vulnerable prisoners. · The needs of the most vulnerable Cameroonians should be prioritised when instituting restrictive and infection control measures. |
|
8. References
Agbor, E., & Tambi, M. (2014). Determinants of HIV/AIDs epidemics prevalence in Cameroon. International Journal of Research and Review, 1(2), Retrieved from: https://pdfs.semanticscholar.org/d617/3d71a0fe84f2a53b10b17937f3a24492ad25.pdf?_ga=2.3968436.506317763.1598029938-1606206363.1598029938 (21/27/2020)
Allegrozzi, I. (2020, May). Covid-19 brings out government's ugly side in Cameroon. Retrieved from: https://www.hrw.org/news/2020/05/14/covid-19-brings-out-governments-ugly-side-cameroon (14/07/2020)
Antonio-Nkondjio, C., Ndo, C., Njiokou, F., et al. (2019). Review of malaria situation in Cameroon: technical viewpoint on challenges and prospects for disease elimination. Parasites and Vectors, 12 (1), 501, Retrieved from DOI: http://doi.org/10.1186/s13071-019-3753-8 (18/07/2020)
APA (Agence de Presse Africaine) (2020, 04 15). Cameroon's health ministry stops daily Covid-19 reports. Retrieved from: http://apanews.net/en/news/cameroons-health-ministry-stops-daily-covid-19-reports (15/07/2020)
ASPR (Assistant Secretary for Preparedness and Response) (2015). The national public health and medical situational awareness strategy implementation plan (2015-2018). Retrieved from: https://www.phe.gov/about/OPP/Documents/phm-sa-ip-sept2015.pdf (25/06/2020)
Bang, H., Mbah, M., Ndi, H., Ndzo, J. (2020) Gauging Cameroon’s resilience to the COVID-19 pandemic: implications for enduring a novel health crisis. Transforming Government: People, Process and Policy, Retrieved from DOI: https://doi.org/10.1108/TG-08-2020-0196 (26/11/2020)
Bang, H., Miles, L., & Gordon, R. (2019). Disaster risk reduction in Cameroon: Are contemporary disaster management frameworks accommodating the Sendai Framework Agenda 2030? International Journal of Disaster Risk Reduction, 10, 462-477, Retrieved from DOI:https://doi.org/10.1007/s13753-019-00238-w (05/04/2020)
Bhattacherjee, A. (2012). Social science research: principles, methods, and practices. Tampa, Florida: Independent Publishing Platform.
Brattberg, E., & Rhinard, M. (2011). Multilevel governance and complex threats: The case of pandemic preparedness in the European Union and the United States. Global Health Governance, 5(1), 1-21, Retrieved from: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=2194169
Bryman, A. (2004). Social research methods (2nd ed.). New York: Oxford University Press.
Cameroon Tribune. (2020, July). Cameroon: Britain supports decentralised testing . Retrieved from: https://www.cameroon-tribune.cm/article.html/32312/en.html/coronavirus-britain-supports-decentralised (18/08/2020)
CDC (Centre for Disease Control and Prevention) (2020). CDC programs in Cameroon pivot to COVID-19 response. Retrieved from: https://www.cdc.gov/globalhealth/stories/cameroon-covid-response.html
Chabrol, F. (2018). Viral hepatitis and a hospital infrastructure in ruins in Cameroon. Medical Anthropology, 37(8), 645-656, Retrieved from DOI: https://doi.org/10.1080/01459740.2018.1518981( 02/08/2020).
Crag, J. (2020, July). UK foreign aid budget cut by £3bn 'due to COVID-19' - as MPs leave for summer recess. Retrieved from: https://news.sky.com/story/uk-foreign-aid-budget-cut-by-3bn-due-to-covid-19-as-mps-leave-for-summer-recess-12034292 (02/08/2020)
CRTV. (2020a, March). COVID-19: Public Health and Communication Ministers face the press with latest facts and figures. Retrieved from: http://www.crtv.cm/2020/03/covid-19-public-health-and-communication-ministers-face-the-press-with-latest-facts-and-figures/ (06/06/2020)
CRTV. (2020b, March). Covid-19: ‘The response mechanism unfolds in four stages’. Retrieved from: http://www.crtv.cm/2020/03/covid-19-the-response-mechanism-unfolds-in-four-stages/ (23/07/2020)
Damme, W., van de Put, Davadasan, N., Ricarte, J., & Muyembe, J. (2018). Is the world ready for the next pandemic threat? British Medical Journal, Retrieved from DOI: https://doi.org/10.1136/bmj.k3296 (28/06/2020)
Djene, E. (2020, March). The Governor of the Littoral bans the consumption of alcoholic drinks in bars. Retrieved from: https://actucameroun.com/2020/04/03/le-gouverneur-du-littoral-interdit-la-consommation-des-boissons-alcooliques-dans-les-bars/ (05/05/2020)
Echouffo-Tcheugui, J., & Kengue, A. (2011). Chronic non-communicable diseases in Cameroon - burden, determinants, and current policies. Globalisation and Health, 7(44), 1-9. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3251529/pdf/1744-8603-7-44.pdf (25/06/2020)
Ekoka, C. (2020). Bamenda: Cameroon Survival Initiative distributes masks and hydroalcoholic gels - COVID-19. Retrieved from: https://cameroonsurvival.org/en/ (14/08/2020)
Emmanuel. (2018). Public Health: Here comes Emergency Operations Centre. Retrieved from: https://www.cameroon-tribune.cm/article.html/22732/fr.html/public-health-here-comes-emergency-operations-centre (12/08/2020)
Epok, G. (2020, April). Coronavirus in Cameroon: compulsory wearing of masks for the populations of the city of Bertoua. Retrieved from: https://actucameroun.com/2020/04/09/coronavirus-au-cameroun-port-obligatoire-des-masques-pour-les-populations-de-la-ville-de-bertoua/ (09/06/2020)
Hammarberg, K., Kirkman, M., & Lacey, S. (2016). Qualitative research methods: when to use them and how to judge them. Human Reproduction, 31(3), 498-501, Retrieved from: DOI: https://doi.org/10.1093/humrep/dev334
HRW. (2020, June). Cameroon: Investigate, distribute health fund. Retrieved from: https://www.hrw.org/news/2020/06/12/cameroon-investigate-distribute-health-fund# (18/08/2020)
Idowu, H. (2020). Understanding governance challenges in Africa. In A. Farazmand, Global Encyclopedia of Public Administration, Public Policy, and Governance (pp. 1-8). Springer, Cham. Retrieved from DOI: https://doi.org/10.1007/978-3-319-31816-5_4013-1
IMF. (2020). IMF Executive Board Approves a US$226 million Disbursement to Cameroon to Address the impact of the COVID-19 Pandemic. Retrieved from: https://www.imf.org/en/News/Articles/2020/05/04/pr20205-cameroon-imf-exec-board-approves-us-226m-disbursement-address-impact-covid19-pandemic (14/08/2020)
IOM. (2020, May). COVID-19 mobility restrictions Cameroon. Retrieved from: https://migration.iom.int (18/08/2020)
IPSOS. (2020a). Responding to COVID-19: highlights of a survey in Cameroon. Retrieved from: https://www.ipsos.com/sites/default/files/ct/publication/documents/2020-05/cameroon_report_0.pdf (19/06/2020)
Kabir, S. (2016). Basic guidelines for research: An introductory approach for all disciplines. Bangladesh: Book Zone Publication.
Kindzeka, M. (2020, May). Cameroon patients flee hospitals as COVID-19 cases increase. Retrieved from: https://www.voanews.com/covid-19-pandemic/cameroon-patients-flee-hospital-covid-19-cases-increase (09/07/2020)
Kouagheu, J. (2020). Cameroon archbishop says treating COVID-19 with plant-based remedy. Retrieved from: https://uk.reuters.com/article/us-health-coronavirus-cameroon-treatment/cameroon-archbishop-says-treating-covid-19-with-plant-based-remedy-idUKKBN23N28K (21/06/2020)
Kouete, V. (2020). Cameroon: 90% of the labour force trapped in the informal sector. Retrieved from: https://blog.private-sector-and-development.com/2020/01/23/cameroon-90-of-the-labor-force-trapped-in-the-informal-sector/ (01/08/2020)
Krishnan, R. (2020, April). ‘Absentee’ Cameroon President reappears after 35 days as opposition demanded a replacement. Retrieved from: https://theprint.in/world/absentee-cameroon-president-reappears-after-35-days-as-opposition-demanded-a-replacement/403549/ (10/05/2020)
Looke, D., Gottlieb, T., & Jones, C. (2015). The global challenges of infectious diseases. The Medical Journal of Australia, 202(5), 225-226, Retrieved from DOI: https://doi.org/10.5694/mja15.00154
Maclean, R., & Marks, S. (2020, April). 10 African Countries Have No Ventilators. That’s Only Part of the Problem. Retrieved from: https://www.nytimes.com/2020/04/18/world/africa/africa-coronavirus-ventilators.html? (28/05/2020)
Madhav, N. (2018). Pandemics: risks, impacts and mitigation . In Jamison, D, H. Gelband, S. Horton, P. Jha, R. Laxminarayan, . . . R. Nugent, Disease control priorities: improving health and reducing poverty, 3rd edition. Washington DC: World Bank
Mbopi-Keou, F.-X., Pondi, J., & Sosso, M. (2020, May). COVID-19 in Cameroon: a crucial equation to resolve. Lancet Infectious Diseases, Retrieved from DOI: https://doi.org/10.1016/ S1473-3099(20)30373-X
MPH (Ministry of Public Health) (2016). Stratégie Sectorielle de Santé 2016 - 2027. Retrieved from: https://www.minsante.cm/site/?q=fr/content/stratégie-sectorielle-de-santé-2016-2027-1(02/08/2020)
MPH (Ministry of Public Health) (2017). Dossier d’investissement pour l’amélioration de la santé de la reproduction, sante de la mère, du nouveau-né, de l’enfant et de l’adolescent/jeune au cameroun. Retrieved from: https://www.globalfinancingfacility.org/sites/gff_new/files/documents/Cameroon_GFF_Investment_Case_Fr.pdf (06/08/2020)
MPH (Ministry of Public Health) (2020a). DONATE. Retrieved from: http://covid19.minsante.cm (28/07/2020)
MPH (Ministry of Public Health) (2020b). Fight against Covid-19: The permanent delegation of the Mfoundi Section of the CPDM has contributed 20,000,000 CFA francs. Retrieved from:https://www.minsante.cm/site/?q=fr/content/lutte-contre-le-covid-19-la-délégation-permanente-departementale-du-rdpc-pour-le-mfoundi (28/07/2020)
MPH (Ministry of Public Health) (2020c, July). COVID-19 MINSANTE Strategy. Retrieved from: http://covid19.minsante.cm (15/06/2020)
MTA (Ministry of Territorial Administration) (2020, April). Press release. Retrieved from: https://www.journalducameroun.com/en/wp-content/uploads/2020/04/New-Doc-04-07-2020-17.24.04.pdf (18/05/2020)
Molem, C. (2008). Decentralisation of health care spending and HIV/AID in Cameroon. In M. Sama, & V.-K. Nguyen, Governing health systems in Africa (p. 256). Dakar, Senegal: CODESRIA.
LeMonde, & AFP. (2020, April). In Cameroon, government wants the funds raised against the virus by opposition leader Kamto to stop. Retrieved from: https://www.lemonde.fr/afrique/article/2020/04/30/au-cameroun-le-gouvernement-veut-l-arret-d-une-collecte-de-fonds-contre-le-virus-lancee-par-l-opposant-kamto_6038237_3212.html (12/6/2020)
Moon, S., Sridhar, D., Pate, M., Jha, A., Clinton, C., Delaunay, S., . . . Piot, P. (2015). Will Ebola change the game? Ten essential reforms before the next pandemic. The report of the Harvard-LSHTM Independent Panel on the Global Response to Ebola. The Lancet, 386(10009), 2204-2221, Retrieved from DOI: https://doi.org/10.1016/S0140-6736(15)00946-0
MSF (Médecins Sans Frontieres) (2020, June). MSF supports COVID-19 response in Cameroon. Retrieved from: https://www.msf.org/msf-supports-covid-19-response-cameroon (11/07/2020)
Nde, C., Raymond, A., Saidu, Y., Cheng, N., Nzoubontane, D., Atemnkeng, J., & Mbacham, W. (2019). Reaching universal health coverage by 2035: Is Cameroon on the track? Universal Journal of Public Health, 7(3), 110-117, Retrieved from DOI: https://doi.org/10.13189/ujph.2019.070304
Ndi, H. and Kimengsi, J. (2017). Mapping epilepsy risks through porcine farming in North West Cameroon, ISABB Journal of Health and Environmental Sciences, 4 (1), 1-10, Retrieved from DOI: http://doi/10.5897/ISABB-JHE2017.0035
NOPH (National Observatory of Public Health) /MPH (Ministry of Public Health) (2017). Life expectancy at birth. Retrieved from: http://onsp.minsante.cm/profiles_information/index.php/Cameroon:Life_expectancy_at_birth/en (07/06/2020)
OCHA (Office for the Coordination of Humanitarian Affairs) (2020, June). CAMEROON: COVID 19 emergency situation report No. 03. Retrieved from: https://reliefweb.int/sites/reliefweb.int/files/resources/cameroon_covid19_emergency_situation_report_no._03.pdf (09/06/2020)
Offner, F. (2020, May). Cameroon: Authorities must urgently protect detainees against COVID-19. Retrieved from: https://www.amnesty.org/en/latest/news/2020/05/cameroon-authorities-must-urgently-protect-detainees/ (14/07/2020)
Ola, E., & Zeger, V. (2020, April). Three lessons in crisis governance for the age of coronavirus. Retrieved from: https://www.weforum.org/agenda/2020/04/a-guide-to-crisis-governance-in-the-age-of-coronavirus/ (01/08/2020)
Papia, A., Skrip, L., Nsoesie, E., Ngwa, M., Abah, A., Galvani, A., & Ndeffo-Mbah, M. (2020). Spatio-temporal dynamics of measles outbreaks in Cameroon. Annals of Epidemiology, 42, 64-72. Retrieved from DOI: https://doi.org/10.1016/j.annepidem.2019.10.007
Potschin-Young, M., Haines-Young, R., Gorg, C., Heink, U., Jax, K. and Schleyer, C. (2018).
Understanding the role of conceptual frameworks: Reading the ecosystem service cascade. Ecosystem Services, 29 (2018) 428-440, Retrieved from: DOI: https://doi.org/10.1016/j.ecoser.2017.05.015
Rapley, T. (2016). Some pragmatics of qualitative data analysis. In D. Silverman, Qualitative Research (pp. 331-347). Los Angeles: Sage.
Reiter, B. (2017). Theory and methodology of exploratory social science research. Human Journals, 5(4), 130-150, Retrieved from: https://scholarcommons.usf.edu/cgi/viewcontent.cgi?article=1134&context=gia_facpub (14/07/2020)
Republic of Cameroon. (2020a). Special statement by Prime Minister, Head of Government of 9 April 2020. Retrieved from: https://www.spm.gov.cm/site/sites/default/files/special_statement_of_the_pmhg_on_the_9_april_2020_scan.pdf (25/06/2020)
Republic of Cameroon. (2020b). Government response strategy to the coronavirus pandemic
(COVID-19). Retrieved from Republic of Cameroon: Prime Minister's Office: https://www.spm.gov.cm/site/?q=en/content/government-response-strategy-coronavirus-pandemic-covid-19 (19/08/2020)
Republic of Cameroon. (2020c). Prime Minister, Head of government announces easing and support measures to relieve the economic sector . Retrieved from: https://www.tralac.org/documents/resources/covid-19/countries/3547-cameroon-governments-covid-19-response-strategy-special-statement-by-the-prime-minister-30-april-2020/file.html (06/08/2020)
Roser, M., & Ritchie, H. (2020). Burden of disease. Retrieved from: https://ourworldindata.org/burden-of-disease#citation (17/08/2020)
SDO (Senior Divisional Officer) (2020a). The Senior Division Officer of Menoua. Retrieved from: https://www.journalducameroun.com/wp-content/uploads/2020/05/Arrete-Pref-Menoua-Covid_30042020.pdf (25/05/2020)
SDO (Senior Divisional Officer) (2020b). The Senior Divisional of Leke Division. Retrieved from: https://www.facebook.com/1226492897398686/photos/a.1303985269649448/2952108818170410/?type=3 (24/05/2020)
Studzinski, N. (2020). Comprehensive pandemic risk management: A systems approach.
Retrieved from: https://www.kcl.ac.uk/policy-institute/assets/Pandemic-risk-management.pdf (12/06/2020)
Tamfu, A., & Lietbouo, A. (2020, June). Feature: Schools in Cameroon gradually reopen amidst COVID-19 pandemic. Retrieved from: XINHUANET: http://www.xinhuanet.com/english/2020-06/02/c_139105960.htm (05/05/2020)
Tih, F. (2020). Cameroon PM meets archbishop over COVID-19 herbal cure. Retrieved from: https://www.aa.com.tr/en/africa/cameroon-pm-meets-archbishop-over-covid-19-herbal-cure/1854713 (28/05/2020)
UN. (2020). World's most vulnerable countries lack the capacity to respond to a global pandemic. Retrieved from: https://www.un.org/ohrlls/news/world’s-most-vulnerable-countries-lack-capacity-respond-global-pandemic-credit-mfdelyas-alwazir (30/07/2020)
UNAID. (2020). Dealing with COVID-19 in Cameroon.
UNICEF. (2020, 04 03). Cameroon Coronavirus (COVID-19) Situation Report No. 5 Internal. Retrieved from UNICEF: https://www.unicef.org/appeals/files/UNICEF_Cameroon_COVID_19_Situation_Report_No.5___10_April_2020.pdf
US Embassy (2018). Ambassador visits Public Health Emergency Operations Center Construction Site. Retrieved from: https://cm.usembassy.gov/ambassador-visits-public-health-emergency-operations-center-construction-site/ (15/08/2020)
USAID. (2017). President's malaria initiative Cameroon Malaria operational plan FY 2017. Retrieved from: https://www.pmi.gov/docs/default-source/default-document-library/malaria-operational-plans/fy17/fy-2017-cameroon-malaria-operational-plan.pdf?sfvrsn=6 (17/05/2020)
Waal, A. (2020). Governance implications of epidemic disease in Africa: updating the agenda for COVID-19. Retrieved from: https://www.lse.ac.uk/international-development/Assets/Documents/ccs-research-unit/Conflict-Research-Programme/crp-memos/Governance-implications-of-epidemics-April-2020.pdf (11/08/2020)
White, G., Thomas, J., Weldon, P., Lawrence, A., Galatis, H., & Tyndall, J. (2013). Grey literature in Australian education. The Grey Journal: an international journal on grey literature, 9(2), 10-108, Retrieved from: https://pdfs.semanticscholar.org/2f47/7b0c9f1835f54e9bb4190ce0d966c5cfc6cf.pdf (28/07/2020)
WHO. (2008). International health regulations (205) (Vol. 2). Geneva, Switzerland: World Health Organisation. Retrieved from: https://www.who.int/ihr/publications/9789241596664/en/ (10/05/2020)
WHO. (2016). Health analytical profile : Cameroon - 2016. Retrieved from: https://www.afro.who.int/publications/health-analytical-profile-cameroon-2016 (23/04/2020)
WHO. (2018). Communicating risk in public health emergencies: A WHO guideline for emergency risk communication (ERC) policy and practice. Retrieved from: https://apps.who.int/iris/bitstream/handle/10665/259807/9789241550208-eng.pdf?sequence=2 (12/04/2020)
World Bank (2020a). Cameroon. Retrieved from: https://data.worldbank.org/country/cameroon?view=chart (28/07/2020)
World Bank, (2020b). Pandemic preparedness and COVID-19. Retrieved from: https://www.worldbank.org/en/topic/pandemics (14/07/2020)
Zamo-Akono, C., Ndjokou, M. and Song-Ntamack, S. (2013). Institutions and hospital efficiency in Cameroon: A data envelopment analysis. Journal of African Development, 15 (1), 45-71, Retrieved from: https://ideas.repec.org/a/afe/journl/v15y2013i1p45-71.html (18/04/2020)
